Predictors of the Best Outcomes Following Minimally Invasive Surgery for Grade 1 Degenerative Lumbar Spondylolisthesis
- There have been conflicting conclusions regarding the benefits of the addition of fusion to decompression for grade one lumbar spondylolisthesis in two recent randomized control trials and a prospective registry study.
- It is possible that evaluation of certain subgroups may clarify these results, and thus the authors of this study evaluated patients who received minimally invasive (MIS) procedures for grade one degenerative lumbar spondylolisthesis.
- Data were obtained from the prospective, multicenter quality outcomes database (QOD) registry of patients who underwent surgery via MIS techniques, defined as MIS laminectomy, MIS pedicle screws, and/or interbody grafts, or techniques that are considered less invasive than traditional, open, and posterior-based approaches (ie, anterior and lateral procedures).
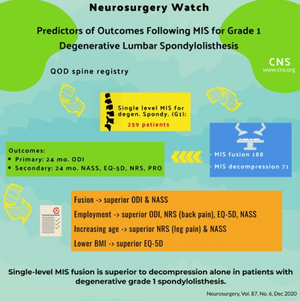
- A total of 259 patients from the QOD lumbar spondylolisthesis module underwent single-level surgery for degenerative grade 1 spondylolisthesis with MIS techniques (188 fusions, 71 MIS decompression alone).
- Demographic, clinical and surgical variables were collected to determine their effects on primary and secondary outcomes.
- Primary outcome was 24-month Oswestry Disability Index (ODI) change. Secondary outcomes included the 24-month North American Spine Society (NASS) satisfaction questionnaire, and 24-month EuroQoL-5D (EQ-5D) change, Numerical Rating Scale (NRS) back pain change, and NRS leg pain change. These were all considered patient-reported outcomes (PRO)
- Multivariate analysis demonstrated that greater baseline PRO severity scores were associated with greater improvements after surgery for each respective PRO.
- Superior ODI change and NASS satisfaction were associated with the addition of fusion in MIS procedures.
- Superior ODI change, superior NRS back pain change, EQ-5D change, and NASS satisfaction were also associated with employment.
- Superior NRS leg pain change and NASS satisfaction were associated with increasing age.
- Lower BMI, as a continuous variable, was predictive of superior EQ-5D change. BMI of 33.89 was identified as the optimal BMI cutoff in the classification tree analysis of reaching EQ-5D minimal clinically important difference (MCID).
- It has been suggested that the potential advantage of fusion for grade one spondylolisthesis may be diminished when evaluating MIS approaches alone as MIS decompression may decrease disruption of soft tissue, however this analysis suggests that the addition of fusion remains beneficial.
